Dental Occlusion
In a dental context, means simply the contact between teeth. More technically, it is the relationship between the (upper) maxillary and (lower) mandibular teeth when they approach each other, as occurs during chewing or at rest.
There are dentists who believe that they can go through their working lives with scant regard for their patients’ occlusion. They seem to believe that essentially they can conduct their practice ignoring the occlusal consequences of the treatments that they perform daily. Whereas all dentists know of the importance of the good marginal adaptation of their restoration to the health of the adjoining dental and periodontal tissues, some dentists do not appreciate the potential consequences of poor occlusal contact to the opposing teeth and their supporting structures.
This can lead some dentists to advocate occlusion as being the key to resolving or preventing a range of disorders far removed from the masticatory system, for example prolapsed lumbar discs. Often such enthusiastic fervour is associated with a didactic prescription of ‘occlusal rules’ which must be adhered to in the treatment of every patient.
The danger is that both of these approaches lead to inappropriate levels of patient care; patients suffer through either over or under treatment.
All patients are different, reacting to similar stimuli in different ways. So the detail of a patient’s individual needs can and should be left to the individual clinician.
But because of the inescapable fact that almost all dental treatment has an occlusal consequence, it is wrong to consider the study of the articulatory system to be less important.
When one considers how almost all forms of dental treatment have a potential for causing occlusal change, the need to establish what constitutes good occlusal practice is overwhelming and obvious.
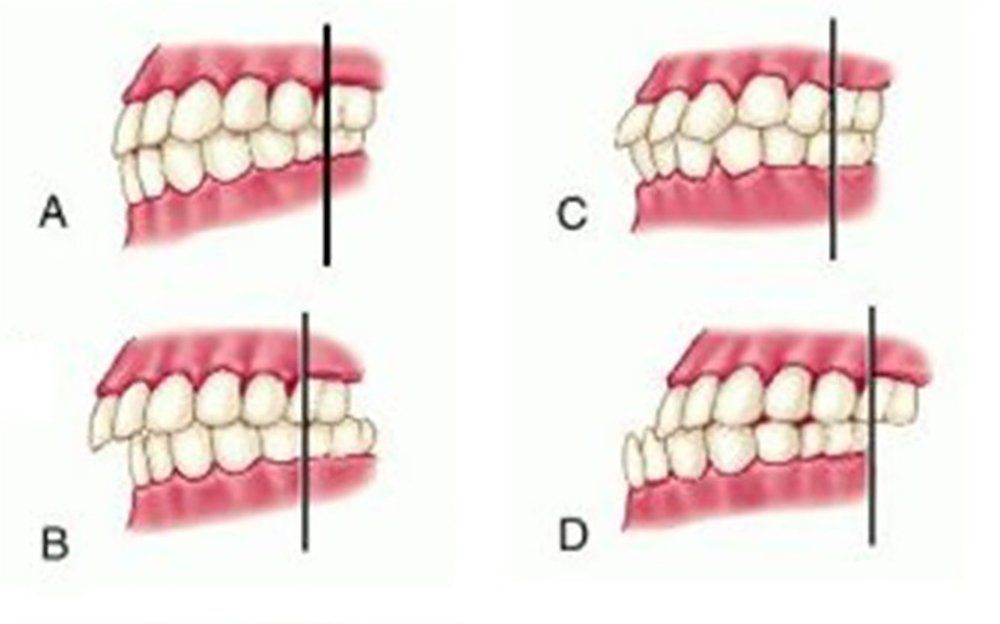
What causes changes in dental occlusion?
- Tooth extraction without subsequent restorative dentistry
This is probably the most common cause of tooth movement and is well known to all dentists. The result of removal of teeth without any placement of restorations to avoid surrounding or opposing tooth movement often results in significant tooth movement in all directions. Such movement is usually nearly impossible to return to a normal state.
- Dental carious lesions develop on the occlusal and proximal surfaces these conditions , allow teeth to drift both occlusally and proximally with resultant collapse of occlusion.
- Wear of teeth
Many patients in any typical general practice have bruxism or clenching habits. These patients have occlusal collapse, their teeth move mesially, and incisal guidance and canine rise increase (clenching) or decrease (bruxism). The result of these changes makes rehabilitation of occlusion in middle age very difficult because of extreme tooth wear.
- Periodontal disease
As the periodontium decreases in support as a result of ongoing periodontal disease, the teeth become mobile. They move in every direction, often allowing occlusal collapse.
- Latrogenic dentistry
Unfortunately, dentists have bad days just like people in other professions. Restorations are often left too high or too low or without adequate contact relationships. These conditions stimulate tooth movement. Dentists can inadvertently cause negative conditions related to occlusion. To reduce the probability of this condition is important to verify the dentist experience, while longer the experience is the lower probability to suffer this condition.
- Diet
Many people eat highly abrasive foods that wear teeth aggressively. Consumed routinely, such foods cause occlusal change
- Traumatic accidents
These occur frequently and cause major changes in occlusion due to tooth avulsion, teeth pushed into supporting bone, broken facial or jaw bones, temporomandibular joint damage, and broken teeth.
- Skeletal growth differences
Variations in skeletal growth or pathological skeletal growth
Symptoms of bad dental occlusion
- Excessive tooth wear
- Tooth breakage
- Tooth loss
- Root canals needs
- Tooth sensitivity
- Head and neck muscle pain
- Headaches
- Jaw joint pain
- Joint noises
- Chronic headaches
- Temporomandibular joint disorder (TMJ)
- Muscle pain
- Tooth movement
- Tooth loss
- Injuries to the teeth
- Tooth wear
- Tooth sensitivity
Oclusión Dental
En contexto dental, significa simplemente el contacto entre los diente. Más técnicamente, es la relación entre los dientes maxilares (superior) y mandibulares (inferior) cuando se aproximan entre si, como ocurre durante la masticación o al descansar.
Hay dentistas quienes piensan que pueden ir a través de su vida laboral con escasa consideración por la oclusión de sus pacientes. Parece ser que consideran que pueden esencialmente conducirse en su práctica ignorando las consecuencias oclusales de los tratamientos que realizan diariamente. Mientras todos los dentistas conocen la importancia de una buena adaptación marginal en sus restauraciones, para la salud de los tejidos periodontales adyacentes, algunos dentistas no aprecian las posibles consecuencias de una contacto oclusal pobre de los dientes opuestos y sus estructuras de soporte.
Esto puede guiar a algunos dentistas a propugnar la oclusión como la clave para resolver y prevenir una serie de trastornos bastante alejados del sistema masticatorio, por ejemplo el prolapso de discos lumbares.
Muy a menudo un fervor tal entusiasta es asociado con una prescripción didáctica de “reglas” oclusales que deben ser agregadas al tratamiento de cada paciente.
El peligro es que ambos de estos enfoques lleva a un inapropiado cuidado a los pacientes; los pacientes sufren de excesivo o muy pobre tratamiento.
Todos los pacientes son diferentes, reaccionan de forma diferente a estímulos similares. Por tanto los detalles de las necesidades individuales de cada paciente pueden y deberían dejarse a cada clínica. Pero por debido al hecho ineludible que casi todo tratamiento dental tiene una consecuencia oclusal, es erróneo considerar que el estudio del sistema masticatorio es menos importante. Cuando uno considera como casi todas las formas de tratamiento dental tienen potencial para causar cambio oclusal, la necesidad de establecer que constituye buenas prácticas oclusales es abrumadora y evidente.
¿Qué causa cambios en la oclusión?
Extracción dental sin subsecuente restauración dental
Esta es probablemente la causa más común de movimiento de dientes y es bien conocida por todos los dentistas. El resultado de remover dientes sin la colocación de ninguna restauración para evitar el movimiento de los dientes que rodean u opuesto muy a menudo resulta en un significativo movimiento en todas las direcciones. Este movimiento es casi imposible revertirlo a su estado normal.
Lesiones de caries dentales desarrolladas en las superficies oclusales y proximales. Estas condiciones permiten que los dientes se desplacen en ambos sentidos occlusal y proximal resultando en un colapso de la oclusión. Desgaste dental Muchos pacientes en cualquier clínica en general padece bruxismo o el habito de apretar los dientes. Estos pacientes padecen un colapso oclusal, su movimiento dental de la línea mesial, canina e incisiva aumenta (al apretar) o disminuye (al bruxar). El resultado de estos cambios provoca que la rehabilitación en adultos de mediana edad sea muy difícil debido al desgaste extremo de los dientes.
Enfermedades periodontales
A medida que el periodonto disminuye en apoyo como consecuencia de la enfermedad periodontal en curso, los dientes se vuelven móviles. Los dientes se mueven en toda dirección, con frecuencia permitiendo el colapso oclusal.
Odontología iatrogénica:
Desafortunadamente, los dentistas tienen días malos al igual que en cualquier otra profesión. Cuando las restauraciones se dejan muy altas o muy bajas o con inadecuado contacto con los otros dientes, se crea estimulación para que exista movimiento en este diente. Los dentistas pueden causar inadvertidamente condiciones negativas relacionadas a la oclusión. Por ello es importante la experiencia que tenga el dentista, mientras mayor experiencia tenga menor probabilidad de sufrir esta condición habrá.
Dieta
Muchas personas consumen alimentos altamente abrasivos que desgastan los dientes en gran manera. Consumir de forma regular esta clase de alimentos provoca cambios en la oclusión.
Accidentes traumáticos
Esto ocurre con frecuencia y causa mayores cambios debido a la avulsión, dientes empujados dentro del hueso que los soporta o hueso alveolar o facial quebrado, daño en la articulación temporomadibular, y dientes quebrados. Diferencia en el crecimiento
Esqueletal
Variantes en el crecimiento esqueletal o crecimiento esqueletal patológico, el resultado de personas altas reproduciendo con personas pequeñas puede ser niños con patrones anormales de crecimiento esquelético. Estos niños por lo general tienen patrones oclusales peculiares y subsecuente oclusión anormal y movimiento dentario.
Síntomas de mala oclusión dental:
- Excesivo desgaste dental
- Fractura de dientes
- Pérdida de dientes
- Necesidad de endodoncias
- Sensibilidad dental
- Dolores de cabeza y en músculos del cuello
- Dolor en articulación temporomandibular
- Ruidos en la ATM
Si se deja sin tratamiento, la mala oclusión puede llevar a:
- Dolores de cabeza crónicos
- Trastornos de la ATM
- Dolor muscular
- Movimiento dentario
- Pérdida dental
- Daños en los dientes
- Desgaste dental
- Sensibilidad dental
Si usted sufre algunos de estos síntomas o sospecha que sufre de mala oclusión contacte a un especialisgta para dar tratamiento y prevenir cualquier posible complicación, en Lorenzana & Dental Associates nuestros especialistas ampliamente cualificados cuentan con vasta experiencia en cada ares, contáctenos info@lorenzanadds.com Tel.1-800-783-0198